: Why It’s Non-Negotiable")
The cycle is over. You’re bigger, leaner, and stronger than ever. You feel great, so why would you need to take more drugs to ‘recover’? This dangerous line of thinking has ruined more hormonal systems than any steroid itself. The truth is stark: Post-Cycle Therapy isn’t something you do after your cycle – it’s the final, most critical phase of your cycle.
To skip PCT is to leave a construction project without a roof – everything you’ve built is vulnerable to collapse. This guide will explain why PCT is non-negotiable for anyone using suppressive compounds like SARMs or steroids, building on the foundation we established in our responsible performance enhancement guide.
The “Why”: Understanding the Biological Crash
The HPTA Simplified: Your Body’s Hormonal Thermostat
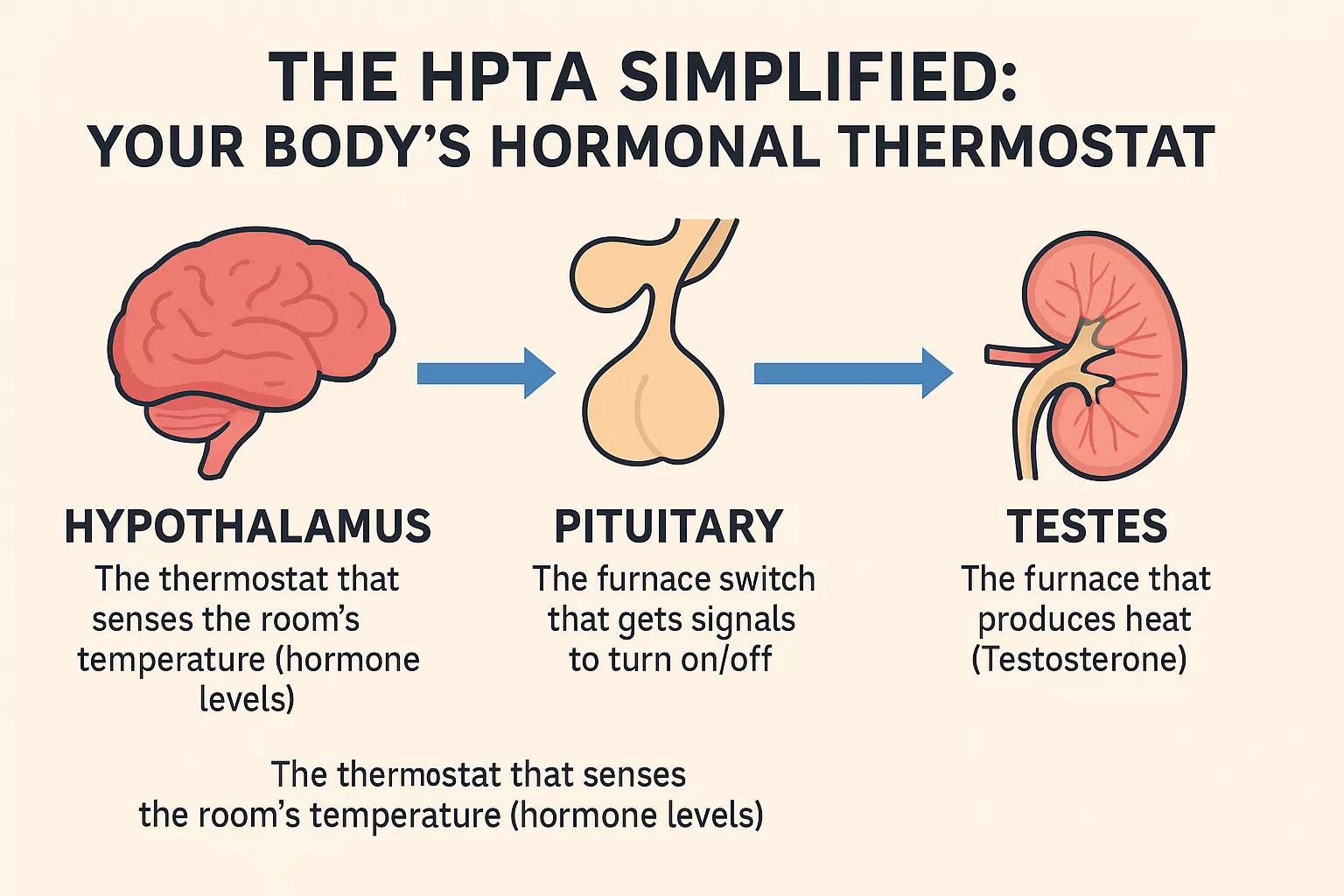
Think of your endocrine system as an intricate heating system:
- Hypothalamus: The thermostat that senses the room’s temperature (hormone levels)
- Pituitary: The furnace switch that gets signals to turn on/off
- Testes: The furnace that produces heat (Testosterone)
When you introduce external hormones, it’s like bringing a space heater that floods the room with heat. Your thermostat (hypothalamus) shuts off, and your furnace (testes) goes cold. This shutdown is called suppression.
What “Crashed” Hormones Actually Feel Like
Without PCT to restart your natural systems, you may experience:
- Crushing fatigue and loss of motivation
- Disappearing libido and sexual function
- Depression and mood swings
- Rapid loss of muscle gains and strength
- Risk of long-term hypogonadism
The National Institutes of Health confirms that hormonal balance is crucial for numerous bodily functions, making recovery essential.
The PCT Arsenal: How Recovery Medications Work
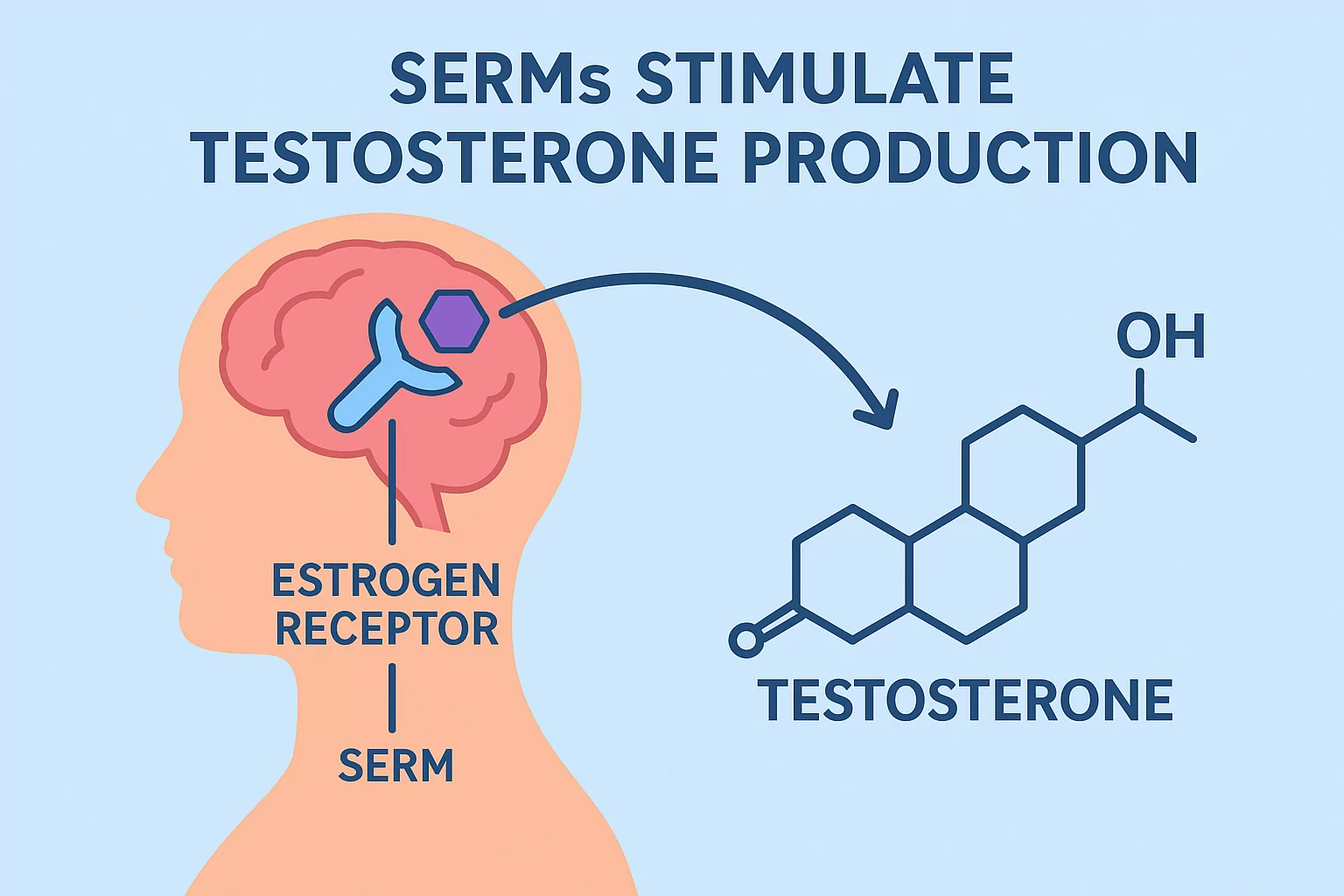
SERMs: The “Wake-Up Call” for Your System
Selective Estrogen Receptor Modulators (SERMs) are the cornerstone of most PCT protocols:
- Tamoxifen (Nolvadex): The reliable workhorse that’s excellent for blocking estrogen in breast tissue (preventing gynecomastia) while stimulating LH/FSH production
- Clomiphene (Clomid): A powerful stimulator that’s often more effective at triggering LH release, though some users experience mood-related side effects
hCG: The “Bridge” Between States
Human Chorionic Gonadotropin (hCG) mimics LH, directly stimulating the testes to produce testosterone:
- Best Used: During the cycle or in the brief gap before SERMs begin
- Primary Benefit: Prevents testicular atrophy and makes the SERM “wake-up call” more effective
- Important Note: hCG is a tool for minimizing the crash, not a replacement for SERMs
Beyond the Drugs: The Forgotten Pillars of Recovery

Pillar 1: Strategic Lifestyle & Nutrition Support
While SERMs restart your hormonal engine, these elements provide the fuel:
- Cortisol Management: Intense training while suppressed skyrockets cortisol. Implement mandatory deload weeks with 50-60% of your normal volume
- Nutritional Building Blocks: Ensure adequate intake of Zinc, Magnesium, Vitamin D, and healthy fats (cholesterol is the precursor to testosterone)
- Sleep & Stress: The HPTA is highly sensitive to poor sleep and high stress – make 7-9 hours of quality sleep non-negotiable
Pillar 2: Intelligent Training & Mental Preparation
Your mindset and training approach must adapt:
- The “Superman is Gone” Reality: You are not as strong or resilient during PCT. Adjust training volume and intensity to prevent injury and support recovery
- Psychological Preparation: Expect a mental dip. Feeling flat, less motivated, and watching the scale drop (largely water and glycogen) is normal and temporary
The Non-Negotiable PCT Protocol: Action Plan
The Essential Prerequisites
Before considering any cycle, you must have:
- Pre-Cycle Blood Work: You cannot know if you’ve recovered without a baseline
- PCT Compounds On Hand: Never start a cycle without having your entire PCT protocol ready
Timing is Everything
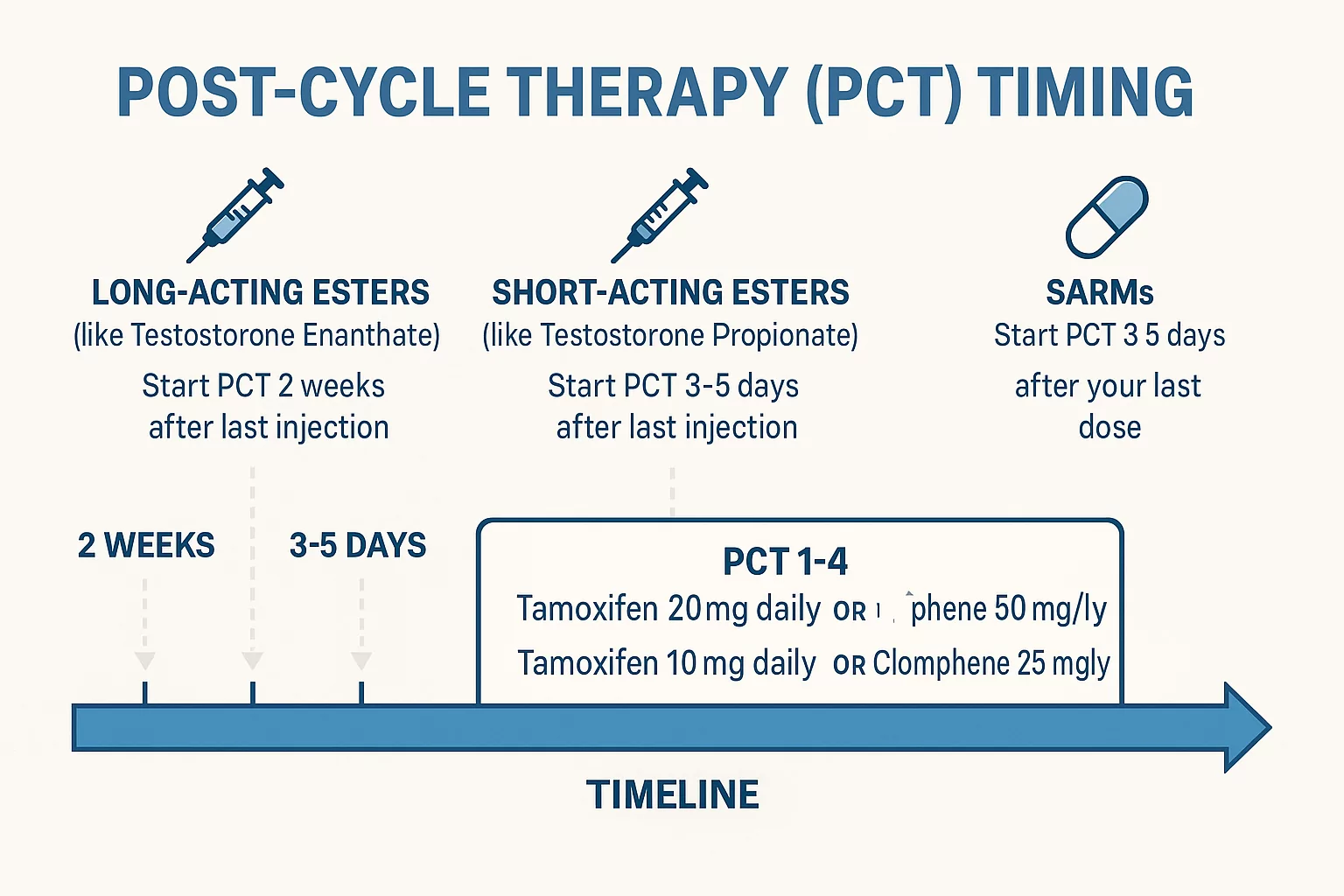
The biggest mistake is incorrect timing:
- Long-Acting Esters (like Testosterone Enanthate): Start PCT 2 weeks after last injection
- Short-Acting Esters (like Testosterone Propionate): Start PCT 3-5 days after last injection
- SARMs: Start PCT 3-5 days after your last dose
Sample Protocol Templates
(Note: These are educational examples, not medical advice)
Basic SERM-Only PCT (for a testosterone-only cycle):
- Weeks 1-4: Tamoxifen 20mg daily OR Clomiphene 50mg daily
- Weeks 5-6: Tamoxifen 10mg daily OR Clomiphene 25mg daily
Advanced hCG + SERM PCT (for more suppressive cycles):
- During cycle: hCG 250-500 IU twice weekly (controversial, but common)
- Between last injection and SERMs: hCG 500 IU daily for 10 days
- Then begin SERM protocol as above
The Final Measure: Post-PCT Blood Work
The only way to confirm successful recovery is through post-PCT blood work, typically taken 4-6 weeks after completing your PCT protocol. Compare these results to your pre-cycle baseline to ensure your natural production has fully restored.
This comprehensive approach to PCT applies whether you’re recovering from a SARM cycle or more traditional anabolic compounds. The principles of hormonal recovery remain consistent across suppressive compounds.
The Final Word: Your Future Self Will Thank You
The true goal of any cycle isn’t just the 12-16 weeks you’re enhanced – it’s the new, improved, and healthy baseline you maintain afterward. PCT is the insurance premium you pay on the house you just built. You wouldn’t skip homeowners insurance to save money, because the cost of a disaster is catastrophic. Your endocrine system is that house.
If you’re not prepared to execute a disciplined PCT with the same commitment you put into your training and diet, you’re not prepared to run a cycle. It’s truly that simple.